Choosing the right insulin regimen is a key decision for people living with diabetes. Among many available formulations, Novolin 70/30 is a commonly used premixed insulin. But how does it compare with other insulin types — rapid-acting, basal (long-acting), analog mixtures, etc.? Which formulation may suit your needs best?
This article breaks down:
-
What Novolin 70/30 is (mechanism, pros/cons)
-
The major categories of insulin (rapid, short, intermediate, long, premixed)
-
How Novolin 70/30 stacks up vs other insulin types
-
Key decision criteria: lifestyle, blood sugar patterns, risk of hypoglycemia, costs
-
How to evaluate “which is right for you”
-
Caveats, transition tips, and when to talk to your clinician
What Is Novolin 70/30?
Composition and Mechanism
Novolin 70/30 is a premixed (fixed-ratio) insulin that combines two distinct human insulin types in a single formulation:
-
70% NPH insulin (isophane, intermediate-acting)
-
30% regular human insulin (short-acting)
Because of this combination, Novolin 70/30 delivers both a short-acting component to cover mealtime glucose surges and an intermediate component that provides basal (background) insulin effect between meals.
Pharmacokinetics (Onset, Peak, Duration)
-
The onset of action for Novolin 70/30 is typically around 30 minutes after injection (reflecting the regular insulin component)
-
The peak activity occurs when both components act: the regular insulin peaks (2–3 hours) and the NPH peaks (4–12 hours)
-
Duration is generally 12 to 24 hours, but the effective tail depends on individual metabolism and dose
Because of the mixed nature, you typically take Novolin 70/30 about 30 minutes before a meal to match the onset with postprandial glucose rise.
Advantages & Limitations of Novolin 70/30
Pros:
-
Convenience: single injection rather than separate short + intermediate insulins
-
Cost: human insulins like Novolin often cost less relative to insulin analogs
-
Predictability for many stable patients
Cons / Challenges:
-
Less flexibility: fixed ratio means you can’t independently adjust basal vs bolus
-
Risk of mismatched peaks causing hypoglycemia or hyperglycemia
-
Less ideal for patients with unpredictable meals or erratic schedules
-
May not provide optimal postprandial glucose control compared to rapid analogs
Also, the FDA label warns not to mix Novolin 70/30 with other insulins or liquids, and to rotate injection sites to avoid lipodystrophy.
Overview: Types of Insulin
To understand how Novolin 70/30 fits into the broader landscape, here’s a primer on insulin classes.
Insulin Classification by Speed & Duration
According to sources like the CDC and ADA, insulins are categorized by onset, peak, and duration.
-
Rapid-acting (bolus): onset ~10–20 minutes, peak ~1 hour, duration 2–4 hours (e.g. insulin lispro, aspart, glulisine)
-
Short-acting (regular human insulin): onset ~30–60 min, peak ~2–3 hours, duration ~5–8 hours (e.g. Novolin R)
-
Intermediate-acting (NPH / isophane): onset 1–4 hours, peak ~4–12 hours, duration ~12–18 hours (e.g. Novolin N)
-
Long-acting / Basal: onset few hours, relatively flat profile, duration up to 24 hours or more (e.g. insulin glargine, detemir, degludec)
-
Ultra-long acting: extended duration beyond 24 hours (e.g. insulin degludec, insulin icodec)
-
Premixed / Mixed formulations: fixed combinations of short/rapid + intermediate insulins, such as 70/30, 75/25, or analog mixtures (e.g. Novolog Mix, Humalog Mix)
These categories allow clinicians to tailor insulin regimens to mimic physiological insulin patterns.
Human Insulins vs Insulin Analogs
-
Human insulins are formulations that replicate naturally occurring human insulin (e.g. regular insulin, NPH).
-
Insulin analogs are molecularly modified to alter absorption kinetics, reduce variability, or flatten peaks (e.g. insulin lispro, aspart, glargine, degludec).
Compared to human insulin, analogs may start working sooner, have smoother profiles, and lower risk of hypoglycemia in some studies, though not always conclusively.
Examples of Popular Insulin Types / Brands
Here are some common examples:
-
Rapid-acting analogs: insulin lispro (Humalog), insulin aspart (NovoLog), insulin glulisine (Apidra)
-
Short / regular: Novolin R, Humulin R
-
Intermediate (NPH): Novolin N, Humulin N
-
Long-acting / basal: insulin glargine (Lantus, Basaglar), insulin detemir (Levemir), insulin degludec (Tresiba)
-
Premixed analogs: Novolog Mix 70/30 (aspart protamine + rapid aspart)
-
Ultra-long: insulin icodec (once-weekly)
How Novolin 70/30 Compares With Other Insulin Types
Let’s compare how Novolin 70/30 fares across several dimensions when set against other insulin options.
Flexibility & Titration
-
Novolin 70/30: Because it is a fixed ratio, adjusting basal vs bolus requires changing total dose and may shift both components in tandem. This reduces fine-tuning.
-
Basal + bolus regimens (using separate basal and rapid/short insulins): More flexibility in adjusting morning vs evening basal, and tuning meal doses independently.
-
Analogs & premixed analogs: Some premixed analogs (e.g. Novolog Mix) may allow slightly better postprandial control while retaining some convenience, though still limited compared with separate basal + bolus.
Postprandial Glucose Control
-
Rapid-acting analogs (lispro/aspart) are faster in onset, better matching meal carbohydrate absorption, reducing post-meal spikes.
-
Novolin 70/30’s regular insulin component is slower than analogs, which may lag behind peak meal glucose, particularly with high-carb meals.
-
In head-to-head, premixed analogs often yield better postprandial control than human-insulin premixes, though individual results vary.
Hypoglycemia Risk
-
The dual peaks of Novolin 70/30 present risk: if basal and bolus needs misalign, one peak might cause low blood sugar.
-
Analogs often have reduced intra-individual variability and smoother profiles, which may lower hypoglycemia risk, especially nocturnal hypoglycemia.
-
Because human insulins are more variable, close monitoring is required.
Stability and Cost
-
Human insulin formulations like Novolin are generally lower cost and more accessible, particularly in resource-limited settings.
-
Analogs tend to be more expensive, though they may offer advantages in management and quality of life.
-
Premixed insulin analogs may provide a middle ground at moderate cost, albeit still costlier than human insulin mixes.
Clinical Use & Indications
-
Novolin 70/30 is approved for use in both type 1 and type 2 diabetes in various regions.
-
It is often used when patients seek reduced injection burden or simpler regimens.
-
However, when precise, intensive control is needed (e.g. in type 1, pregnancy, erratic schedules), basal + bolus regimens with analogs may be preferred.
Safety and Practical Considerations
-
Always rotate injection sites to avoid lipodystrophy.
-
Do not mix Novolin 70/30 with other insulins or liquids.
-
Check compatibility, shelf life, storage (e.g. refrigeration) per insulin label.
-
Transition from one insulin regimen to another should be managed under clinical supervision due to risk of misdosing.
Which Insulin Type Might Be Right for You?
Choosing the best insulin regimen is a personalized decision. Below are key factors to consider.
1. Blood Sugar Patterns & Glucose Variability
-
If your fasting, pre-meal, and post-meal glucose patterns are predictable, a premixed insulin like Novolin 70/30 may suffice.
-
If you experience large post-meal peaks or variable responses, more adjustable regimens (basal + bolus) may perform better.
2. Lifestyle and Meal Regularity
-
If you eat meals at regular times, the fixed action profile of Novolin 70/30 may fit well.
-
If your schedule is irregular (meals at variable times, shift work, travel), you may prefer faster analogs and flexible dosing.
3. Injection Burden & Simplicity
-
A premixed insulin is simpler (fewer injections), which can improve adherence for some patients.
-
But simplicity trades off flexibility — you sacrifice some tuning ability.
4. Risk Tolerance for Hypoglycemia
-
If you are at higher risk (e.g. elderly, renal impairment), a regimen with smoother insulin profiles (analogs, basal + bolus) might reduce hypoglycemia risk.
5. Cost & Access
-
If cost is a limiting factor, human premixed insulins like Novolin 70/30 may be more accessible.
-
Some analog insulins may not be covered by insurance in some settings or may be priced higher.
6. Clinical Context (Type 1, Type 2, Special Populations)
-
In type 1 diabetes, many clinicians favor basal + bolus regimens with analogs for more precise control.
-
In type 2 diabetes, especially when insulin is started later, premixed insulins are often used in simpler regimens.
-
In pregnancy, kidney disease, older age, clinicians may prefer analogs that reduce risk of hypoglycemia.
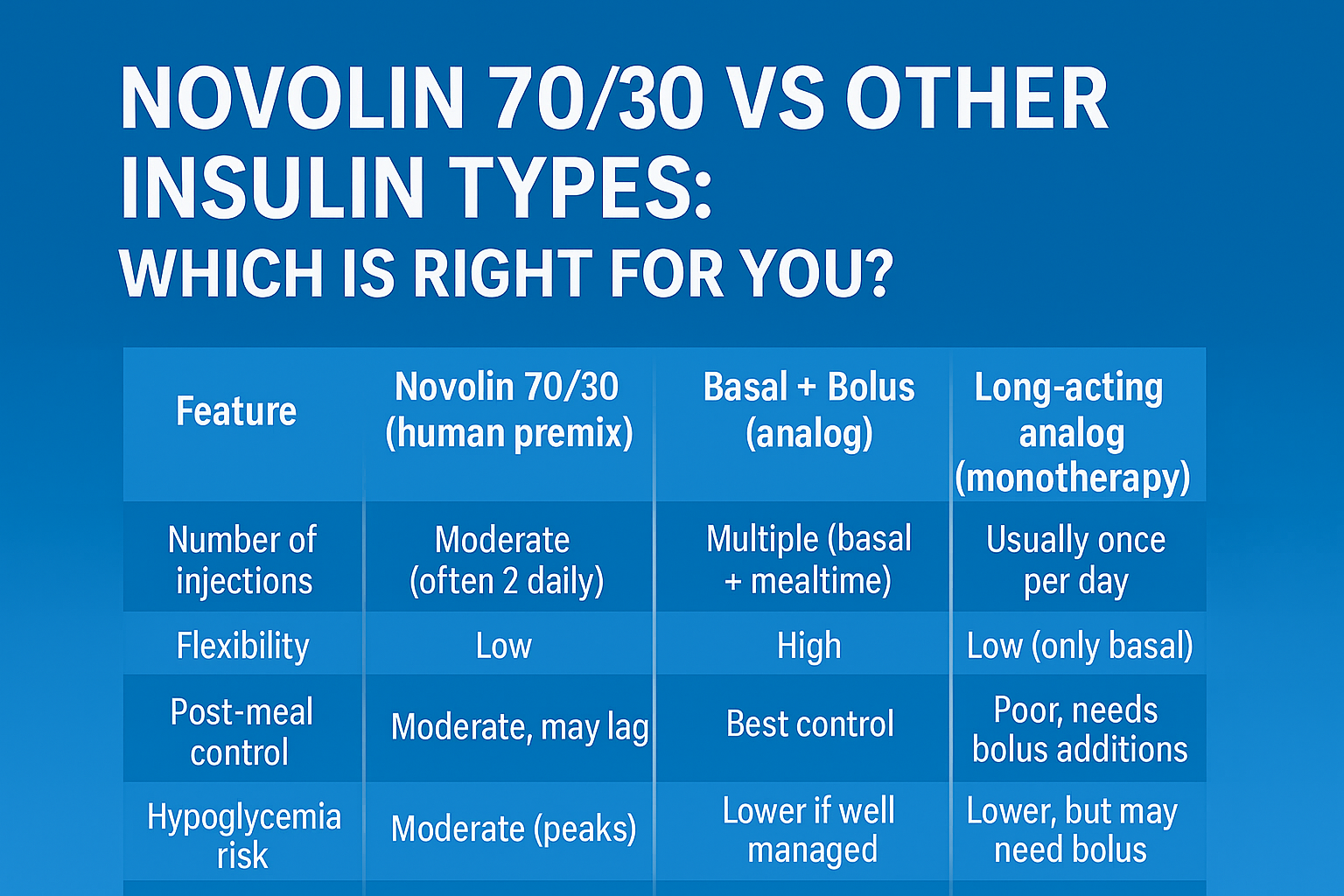
Sample Comparisons
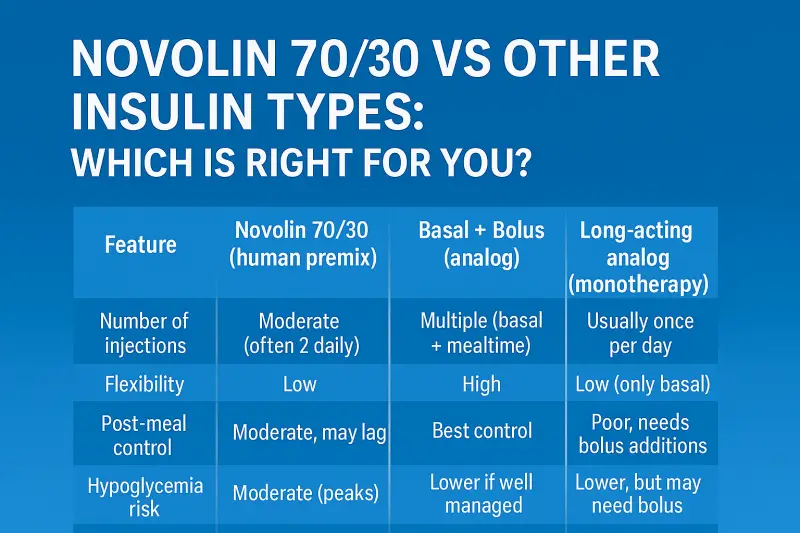
Here’s a tabular summary (simplified) showing how Novolin 70/30 compares with other classes:
| Feature / Insulin Type | Number of injections | Flexibility | Post-meal control | Hypoglycemia risk | Cost | Ideal for |
|---|---|---|---|---|---|---|
| Long-acting analog (monotherapy) | Usually once per day | Low (only basal) | Poor, needs bolus addition | Lower, but may need bolus | Moderate to high | Mild insulin requirement or basal support |
| Basal + Bolus (analog) | Multiple (basal + mealtime) | High | Best control | Lower if well managed | Higher | Intensive control, variable schedule |
| Novolin 70/30 (human premix) | Moderate (often 2 daily) | Low | Moderate, may lag | Moderate (peaks) | Lower | Stable routines, limited resources |
Transitioning and Practical Tips
If you’re considering switching to or from Novolin 70/30, here are practical suggestions:
Initial Dose Estimation & Titration
-
Your clinician might split your current total daily dose into two injections (e.g. 2/3 morning, 1/3 evening), depending on glucose patterns.
-
Monitor glucose levels intensively (fasting, prelunch, predinner) during transition.
-
Adjust slowly — changes in insulin affect both basal and mealtime control.
Timing & Meal Matching
-
Inject ~30 minutes before meals when using Novolin 70/30 to align with onset.
-
Keep consistent carbohydrate intake and timing while adjusting.
Avoid Mixing & Compatibility
-
Do not mix Novolin 70/30 with other insulins or diluents.
-
Always check the insulin label — never assume interchangeability without clinical guidance.
Injection Site Rotation
-
Rotate among abdominal, thigh, buttock, and upper arm sites to avoid lipohypertrophy.
-
Do not use the same exact spot repeatedly.
Monitoring and Adjustments
-
Frequent self-monitoring of blood glucose is essential during changes.
-
Use adjustment algorithms (as your clinician recommends) to fine-tune.
-
Watch for signs of hypoglycemia or hyperglycemia, especially during the first few weeks.
Safety Considerations
-
Be cautious in patients with renal or hepatic impairment (altered insulin metabolism).
-
In older adults, risk of hypoglycemia mandates conservative dosing and close monitoring.
-
In case of illness, stress, or changes in activity, insulin needs may fluctuate.
Real-World Scenarios: What Might Suit You Best?
Here are some hypothetical scenarios illustrating when Novolin 70/30 may or may not be optimal.
-
Scenario A (Good fit for Novolin 70/30): A person with type 2 diabetes, regular 3 meals per day spaced evenly, minimal dawn phenomenon, wants fewer injections and lower cost.
-
Scenario B (Less ideal): A person with type 1 diabetes, frequent snacking or meal-time variation, with history of nocturnal hypoglycemia — may benefit more from basal + rapid analogs.
-
Scenario C (Intermediate case): A person on two daily mixed analogs — perhaps switching to Novolin 70/30 might save cost but may lose some post-meal control; careful monitoring required.
Summary & Take-Home Points
-
Novolin 70/30 is a fixed-ratio mix of 70% NPH (intermediate) + 30% regular (short) human insulin.
-
It offers convenience and lower cost but limited flexibility.
-
Other insulin types—especially regimens combining basal + bolus with analogs—offer more control, flexibility, and potentially lower hypoglycemia risk.
-
The “right” insulin depends on your blood glucose patterns, meal schedule, hypoglycemia risk, resources, and lifestyle.
-
Always make changes under the guidance of a healthcare provider, with close monitoring.
References
-
U.S. Food and Drug Administration (FDA). Novolin 70/30 Prescribing Information.
-
Centers for Disease Control and Prevention (CDC). How to Use Insulin.
-
American Diabetes Association (ADA). Types of Insulin.
-
National Center for Biotechnology Information (NCBI), U.S. National Library of Medicine. Insulin Analogs.
-
ADCES (Association of Diabetes Care & Education Specialists). Insulin Types and How They Work.
-
GoodRx Health. What Is Novolin 70/30?
This article is for informational and educational purposes only. It is not intended to provide medical advice, diagnosis, or treatment. Always seek the guidance of your physician or other qualified health provider with any questions you may have regarding your health, medications, or a medical condition. Never disregard professional medical advice or delay seeking it because of something you have read here.